Now, more than ever, we need to show the value of team-based primary care. Your team can help by sharing your stories via AFHTO’s QI enablers study. AFHTO members have gained the respect of many through their high and ongoing participation in D2D. It is not enough to just measure, though. The next step is to use that data to explore if and how relationship-based primary care is also better care, as Starfield’s work suggests. We need to learn more about how teams run their shops and use their data, so we can see what kinds of structures and processes make a difference in performance. This can give us all bigger hints about what to try to get to better outcomes for all teams. If we can pull this off, it would make a very clear case for the value of team-based care. Here is what you can do:
Keep measuring: This is the fuel for all kinds of fires to support improvement in, demonstrate value of and advocate for teams!
Extra demand on your time: none if you are already doing D2D.
Extra demand on your time: about 10 minutes if you are already doing D2D.
Tell your peers how you work: Sit down with AFHTO staff to explain how you do what you do in your teams in terms of measuring and improving. This will help teams compare and contrast with one another to find hints to act on, to get to better outcomes.
Extra demand on your time: 4 hours for in-person or phone interviews.
Dive deeper into team functioning: Join a research study looking at what difference integration and collaboration makes on patient outcomes.
Extra demand on your time: 15 minutes for each provider who completes a Provider Questionnaire, which includes the Collaborative Practice Assessment Tool (CPAT) and seven demographic questions. NOTE: You don’t need to get every provider to complete the questionnaire, as long as you can get representation from across the key disciplines in your team (family doctors, nursing staff, and IHPs). If you get 20 staff to participate, that’s about 5 hours of staff time – or the first 15 minutes of a team meeting.
The more data we have, the more we learn. With only a few teams participating, we can’t be sure we’re making the right connections. We need teams from across the province, at all levels of performance and all stages of quality improvement, to help us understand what they are doing and connect it to how they are doing. Want to know more? Send your questions to Carol Mulder, Provincial Lead for the Quality Improvement Decision Support Program.
Information to Action is a collection of resources and tools that teams can use to start improving the quality of care they deliver now. Through Information to Action, we will provide dedicated support to teams interested in using the momentum of D2D to move from measurement to improvement. It is also meant to teach us what really works for all AFHTO members to translate Information to Action. The overall goal is to help teams deliver higher quality care. How will we know if it’s working? Hopefully, we will see the results in the data teams submit to future iterations of D2D.
Who is Information to Action for?
All teams are invited to assess how ready they are to be part of Information to Action. Just like with D2D, not all teams will be ready to make this move right away. And just like D2D, teams can start slowly, taking advantage of only those parts of Information to Action that work for them right now.
Start with the”Free-Choice” resources and activities. These are things your team can start doing now – or may already be doing. They have no prerequisites.
Consider the “Resources with Strings Attached.” These are more intensive supports you might consider signing up for if your team is ready. There is some homework you will have to do to help you prepare for them.
Volunteer to tell the story of your team’s QI journey as part of AFHTO’s QI enablers study. Teams from all stages of the QI journey are needed. This will make it easier to identify which characteristics, processes and tools are truly effective enablers for improving quality.
Access EMR Maturity Development resources from Ontario MD
Sign up for support from the EPEP consultants and/or OntarioMD peer leads to access topic or task-specific support. This support can help you make better use of your EMR in your quality improvement efforts. The EPEP consultants will help teams narrow down their focus to specific tasks that can be achieved in the context of the improvement initiative.
Teams rightfully pride themselves on the relationships they build with patients, but most of the data teams use to demonstrate their value is the number of patients they serve. The PPPC gives you a way to demonstrate the quality, not just the quantity, of service you provide.
Please consider sharing your results with AFHTO staff, to be used as part of the QI enablers and patient priorities studies. Our hope is that teams will have completed their patient-centeredness survey by May 2018.
Access a CME accredited privacy training module and resources through Ontario MD. The module and resources are designed to facilitate your use of technology and ensure accountability that Health Information Custodians have with respect to the appropriate collection, viewing, use, disclosure and safeguarding of personal health information.
Resources with Strings Attached
The resource described below (Lean training and Practice Facilitation training) are more intensive and require some investment on the part of AFHTO and the participating teams. To make sure that everyone gets value out of this investments interested teams will be expected to participate in certain activities, including some of the “free choice” activities described above. At a minimum, teams participating in any of the services below will be asked to do the following:
Develop a team-specific improvement focus. Work with your clinicians, IHPs, QIDS Specialist (if you have one), and anyone else on your team who has an interest in quality improvement. Choose a focus that is manageable and meaningful for your team, appropriate for your setting, and relevant to your patients’ needs.
Administer the Patient Perception of Patient Centeredness Questionnaire (email us to get a copy), and
Participate in an interview later in the Information to Action process to share what changed (if anything) in your team’s area of focus on improvement.
NOTE: Winter 2018 Lean training session has concluded. Stay tuned for future opportunities!
One person from each participating team will be invited to participate in one 5-day on-site training session plus remote coaching for 2 months (up to 6 trainees). The participant will be awarded a Green Belt on completion of the program. Unsure if LEAN training is right for your team? Read more about it here.
Team expectation: In addition to the minimum expectations described above, participating teams may need to cover travel and accommodation for the LEAN trainee. Participating teams will also need to cover tuition for any staff they send for LEAN trainee beyond the 6 positions available. Teams will also be expected to collaborate with their trainee in improving performance in the area of focus identified by the team and the trainee.
LEAN coaching will be available at no charge on a weekly basis for 8 weeks for teams enrolled in LEAN training. Additional coaching may be available at a charge to participating teams beyond the period offered through Information to Action. Join the discussions that launch a Quality Improvement Community of Practice (CoP), focused specifically on QI. It is open to all interested teams, especially those taking advantage of the LEAN training.
You do not have to participate in the LEAN training or coaching to be part of this CoP.
As in other CoPs, members of the community will be supported by facilitators and themselves in navigating available resources such as those listed here and those that might be available in specific LHINs or for specific topics, such as:
Teams interested in topics supported by these various coaching resources (among others) will be introduced to those providing the resources, to make it easier for teams to take advantage of these services.
The CoP will also support teams in monitoring progress against milestones on a monthly basis and/or troubleshooting challenges.
Progress in translating Information to Action: Interested teams may want to review their progress and that of their peers at special forums throughout the year. There may also participate in the orientation of the next cohort of interested participants, tentatively planned for the 2018 AFHTO conference.
Practice Facilitation Training for QIDSS
NOTE: The Practice Facilitation Training sessions are finished. If interested, please consider contacting the Centre for Effective Practice to learn about other opportunities for this.
Offered in partnership with the Centre for Effective Practice (CEP), this is a free, three-day training session in Toronto for QIDS Specialists and other QI professionals (QIDSS-like folks). The course will introduce you to academic detailing, a service that offers one-on-one educational outreach visits to family physicians to discuss objective, evidence-informed ways to improve care quality. By taking part in the training, QIDSS and QIDSS-like folks will be more confident working with clinicians about how to apply evidence and data to their practice. They’ll also learn about the CEP’s academic detailing service and how this could benefit their teams.
Team expectation: In addition to the minimum expectations described above, participating teams may need to cover travel and accommodation for the trainee. There are a limited number of spaces, and these are available on a first-come, first-served basis.
Self-Assessment of Readiness
Interested teams are invited to complete a self-assessment of their readiness to succeed in this initiative by asking themselves the following questions. Once you have completed the self-assessment, send in your answers to us through this online survey..
Have all of our leaders agreed to participate in this initiative?
You know who your leaders are. Are they ready to make sure that the team follows through on their home work?
Do your team’s physicians know what their role is?
Is there at least one physician who agrees to champion the project and encourage other team staff and physicians to participate? If not, is there at least one physician who agrees to accommodate the project and allow access to their staff, patients and/or data as necessary for the project to proceed?
Can you agree on at least one problem you all want to solve?
There is likely no end of things that bother someone or other on your team. Is there one problem (or possibly 2) that you all want to do something about sooner rather than later? You do not need to have a fully defined “QI project” or research question – you will do that as part of this initiative. You just all have to agree that you want to take on this problem.
Does your QIDSS (or similar person) have access to your EMR?
It is almost certain that you will need to get at your EMR data to succeed with this. Administrative staff supporting the initiative (usually QIDSS or similar person) must have be able to extract data from your EMR. Have you got that set up yet or at least in progress?
Are you prepared to do your homework?
Your part in the initiative involves completing some baseline activities to measure and increase your access to data. These activities are listed below. Is your team ready to do these things as best you can?
Plan to take action on at least one area reflected in D2D: Choose an improvement focus based on at least one aspect of your team’s D2D performance, in addition to any other topic you wish to examine.
Share experience: Join your fellow participants to share your experience in various forums such as surveys, one-on-one discussions, focus groups and/or presentation at the next AFHTO annual conference.
Are you still working on getting ready?
Maybe your team wants to do some of your own work first before signing up for this initiative. Perhaps you have other pressing issues. If your team is not yet ready to participate in this improvement initiative, all is not lost. You can still participate in the improvement activities available to all members. You can also work on the criteria above at your own pace. There will likely be additional supports for improvement after the initial cohort for this improvement initiative is completed. The exact nature of the second cohort depends on how things go with the first. In addition, you may be able to make progress on your own even outside the improvement initiative because some of the services/supports are already available to members on request.
Frequently Asked Questions
As they think about signing up for this initiative, members have been asking questions. These are summarized below. They will be updated throughout the planning and implementation of the initiative.
What is the charge for participating?
The supports are free for this first cohort with the possible exception of some travel/accommodation costs for training activities.
How much information should we include in the readiness self-assessment?
The readiness self-assessment is available to help you decide how ready you are, so you can include as much (or as little) information as you like. Keep in mind, only teams who complete the readiness self-assessment will be eligible to participate in the “strings attached” resources.
How do teams sign up for the “strings attached” resources and how are the teams chosen?
Teams were invited to sign up for the “strings attached” resources (LEAN training) after the orientation session at the AFHTO conference. Teams were chosen on a first-come, first-served basis.
What if we don’t have very good performance?
Performance is NOT AT ALL a criterion for participation.
What if our team and our physicians have different priorities?
If the team and physicians are not yet in agreement on a priority problem but can agree on one problem they want to work on together and there is at least one physician who is supportive, you may decide you are ready to give this a try. Or you may decide to take a bit more time to work on getting to that point on your own before you enrol in an initiative like this. Many of the free choice supports are already available to all teams and may be useful in getting over this hurdle.
What if we don’t have a QIDS Specialist?
You don’t need to have a QIDSS to participate. In fact, you may find that that Information to Action will helps you cope without a QIDSS even better than you already are doing. If you don’t have a QIDSS, you will just have to ask someone else on your team to be the point person to support the data access/decision-support functions within your team.
Can we sign up as a group of teams or with non-AFHTO providers?
For sure!
What happens if we don’t improve?
Don’t worry. The goal is to build capacity for improvement activities and learn what it takes to improve. If you have tried something and it hasn’t worked to improve performance, at least you will know one thing NOT to do! As long as there is increased awareness and skill and lessons learned, the program will have met one of its most important goals.
Is this “one and done” or will there be a second cohort?
We hope for many cohorts. Improvement is one of AFHTO’s key strategic priorities. As long as that is true, AFHTO will be in the business of supporting improvement. One of the goals of this first cohort is to learn what it takes to do that well. Supports for future cohorts may or may not look the same as those for this first cohort, depending on what we learn.
What if we don’t want to work on anything in D2D?
Part of the goal is to demonstrate improvement in performance in the next iteration of D2D. To that end, we would prefer teams to choose something relevant to D2D. This will also make it easier to compare progress to others. However, if there really is nothing related to D2D that your team wants to work on, its probably not a deal-breaker to choose something else. Either way, you will be helping achieve the other goals for this initiative ie build capacity for improvement and learn more about what works best to build that capacity. To reach that latter goal, we will evaluate baseline and post-initiative data as well as have much conversation with participants about what worked for them throughout the initiative.
‘Lean thinking’ originated in the automotive sector and is now being utilized by various industries. It is especially valuable in the health care realm, where demand for care continues to grow and budgets are perennially tight, making both effectiveness and efficiency vital. “Lean” gives this industry not just a set of tools to use and procedures to follow, but a comprehensive and integrated thought process, culture and system of beliefs in the pursuit of improved patient care within available resources. The result of Lean Healthcare is a process that delivers value without waste, with high quality, at a low cost. A Lean Tool Box is available to support the elimination of waste and the streamlining of process flows. In health care, one must always remember that the product (laboratory test results or samples) or service (patient care) can make the difference between life and death. The needs of the patient are paramount. The Lean Sigma Green Belt program is designed for Healthcare professionals, to discover ways to implement core Lean concepts, tools and practices to optimize and error-proof care-critical business processes and create ongoing and sustainable improvements. Application of the knowledge and skills gained will improve primary care teams for all staff from those delivering direct care to the Executive Director, as well as the care delivery for all patients. Lean is predicated upon meeting the Voice of the Customer, and the instructors will utilize these principles to deliver relevant participatory curricula grounded in adult learning principles. The objectives for each section of the curriculum are designed according to Bloom’s Taxonomy, maximizing the experience and outcome of learning for each student. Figure 1: Bloom’s taxonomy classifies the objectives that educators set for students into three domains: cognitive, affective, and psychomotor (sometimes loosely described as “knowing/head,” “feeling/heart,” and “doing/hands,” respectively). The delivery method comprises a mix of didactic and interactive portions, triggering the inductive and deductive learning cycles of each student, encouraging the conversion from knowledge to application and analysis of the methodologies, tools and concepts. Moving from passive to active learning, the Lean Six Sigma Green Belt students will be supported to build a Lean skill set that will increase their ability to not only see new opportunities, but to move them to action. Figure 2: Inductive and Deductive Reasoning In addition to a focus on Lean approaches, methodologies and tools, a strong Facilitation component will be designed for the internal improvement facilitators. A module on Change Management to assist the facilitators to engage and coach staff in achieving improvements will also be a feature of the curriculum. Through a learn-by-doing approach, the program will work to mentor the Lean Six Sigma Green Belt students towards building self-starting capability within the organization. The measure of success will be when the candidates are able to design and deliver change independently, in alignment with the goals and objectives of their teams and the strategic objectives of AFHTO. While classroom education can be a useful vehicle for learning, leveraging real projects, a “hands-on” integrated approach to the coaching, mentoring and training of management and staff across an organization is far more effective with respect to knowledge transfer. In line with the Lean approach, focusing purely on financial metrics would not only drive the wrong behaviours, but would also disengage the majority of the workforce. The program will therefore take a balanced approach to opportunity identification using QCAPS (Quality, Cost, Access, People & Safety) in optimizing services for clients and patients. An overall evaluation of each cohort of Lean Six Sigma Green Belts will be performed in consultation with the Leadership team to ensure that projects are aligned with organizational goals.
Five iterations of D2D data show that some teams tend to improve more over time compared to others. AFHTO members want to know what some of the “tricks of the improvement trade” are so they can try them out in their own teams. This QI enablers study is aimed at learning more about what makes it easier or harder to improve so that all teams can take advantage of the wisdom from the field.
The QI Enablers study will be based on in-person interviews with teams. It will provide a snapshot of how teams think and work to get better at what they do. We will ask teams “what works and why” when they try to get better at what they do. Details on the interview process are outlined below. The study will describe what is happening with teams at a single point in time – ie it is not ongoing, the way that D2D is. The data from the interviews (which will mostly be in the form of stories) will be compared to D2D performance. This will point out any patterns between the stories of how teams work and their D2D scores which will provide hints regarding what works best to move beyond measurement to improvement. The key is to have teams from ALL stages of the QI journey so we can compare and contrast. We will share the stories first with the participating teams to confirm that we have heard them right. Then we will be sharing the collective wisdom from the stories with all members and also with external partners, so that everyone (AFHTO members and beyond) can learn together. The stories will be shared anonymously – unless a team is keen to see their name in lights, in which case we would happily oblige!
How will the study be done?
The team visits and interviews will be done by Carol Mulder, Provincial Lead for Quality Improvement and Decision Support and Laura Belsito, Clinical Knowledge Translation and Exchange Specialist, supported by any graduate students we are able to recruit and the QIDS program staff at AFHTO. We will spend about 4 hours at each team site, talking to whoever the team wants us to talk to. We have put together a “straw dog” schedule to give teams a sense of who might be included. However, it is totally up to the team to decide who will meet with us to tell their story. In addition, the conversations can take place in any order the team wants – ie Hour 1 doesn’t have to be the first hour if that doesn’t work for the team.
Hour 1: ED, Medical Lead and Board Chair
Hour 2 (2 groups): Separate conversations with QI staff (QIDSS and others?) and patients
Hour 3: IHPs and physicians together
Hour 4 (2 groups): Separate conversations with clerical staff (including physician staff, if different from FHT clerical staff) and possibly LHIN performance staff
When will the study happen?
Visits to teams will be scheduled starting September 2017. See below for draft timeline. Note that this study will be taking place at the same time as patient focus groups to learn more about patient priorities for primary care measurement (see the patient priorities survey information on the AFHTO web site for more information). Interested teams may choose to volunteer for both the QI enablers visits and a patient focus group if they choose.
Activity
Start
End
Invite teams to participate
NOW!
July 31, 2017
Schedule interviews
August 4, 2017
September 26, 2017
Conduct interviews
September 27, 2017
ongoing
Summarize input
October 30, 2017
January 31, 2018
Reflection with participants and QSC
February 15, 2018
February 22, 2018
Take action
NOW!
April 30, 2018
What we want to talk with teams about
We will visit teams and ask them “what works and why” when they try to get better at what they do. This approach is loosely grounded in theories of “appreciative inquiry”, “solutions focus” and “positive deviance.” In keeping with these theories, the interview questions will follow the stories of the people we are talking to. That means the questions won’t be the same for each person or team we talk to. However, the stories we are looking for are the same for all teams. They include:
Stories about your attempts to get better at something: How did you know you needed to get better? Who decided? What happened when you tried to change things? Who worked on it? How do you know if it worked or not? Who was happy about it? Who wasn’t? Why?
Stories about learning from what you tried in the past: How do you feel now about being able to make something else better? What makes you feel that way?
Stories about the “perfect storm” for improvement: When did it last happen for you? What does it look like? Who is there? What made the storm? Who likes the storm?
Stories about your special skills/people/processes (ie superpowers) for improvement or good primary care: What are they? How did you get them? What do you use them for?
When we are hearing the stories, we will be looking for some particular ideas in the data (see below). Even if they are not there, that might mean something. For example, if nobody talks about how many people need to be on board for improvement to work, that might be as interesting as finding out that teams agree on a certain minimum number.
Drivers for quality improvement
Triggers for improvement
Confidence and appetite for change in the team (improvement = change)
Culture of innovation/tendency to try new things FIRST vs wait for tried/tested solutions
Minimum critical mass of staff to enable improvement (if any)
Role of leadership and/or intentional planning in successful improvement
Absolute requirements for successful improvement (if any)
Role of EMR functionality and data
QI as an approach to work vs a separate project
Significant team events (eg Change in ED) that might affect QI activity
What we won’t ask teams about
Teams will not be asked why they are doing better (or worse) than others in making things better over time. This is partly because they might not know – and partly because it doesn’t matter that much. For example, maybe all (or no?) teams feel they have superpowers. Yet some teams may find it easier to get better than other teams, even if they all have the same superpower. This might mean that superpowers matter for other reasons but might not be the answer we thought they were in terms of making things better.
Frequently Asked Questions
Is this a formal research study? Yes. This is an observational, qualitative cross-sectional study. AFHTO will be getting approval from the Research Ethics Board for it. Why do this as a formal research study? AFHTO Board has recently affirmed its commitment to playing a leadership role in primary care and, more broadly, in the Ontario healthcare sector. AFHTO needs to be able to tell the story of its leadership in a wide variety of forums to demonstrate that leadership. A formal research study (with formal ethical approval) makes it possible to share the collective wisdom of AFHTO members in credible and high profile way to support leadership activity. Do members HAVE to participate? Practically everything AFHTO does is voluntary and intended to serve the members. Members can choose not to be interviewed simply by not volunteering. Nobody but they themselves will ever know that. Can I tell my story to AFHTO but not be in the research study? We will only include the stories of teams who agree to be part of the published study but we will listen to and share ALL the stories among the members for their own use. And all the stories will be anonymous unless a team is keen to have their name in lights, in which case we would happily oblige! What if our team is really struggling to improve? You are so not alone! And your story is really important. You may be doing everything “right” and still be in the place you are. That is the kind of story that will help us all see what actually is important on the ground (vs in theory). If we only talk to teams who are making good progress, we will not get useful information for those who are in the trenches, pulling out all the stops and still frustrated. You (all of you!) really are the answer! Who should be part of the interviews? Bring whoever you want to the table. We have a hunch about some roles that tend to be important in a team’s efforts to get better – see our list above. You may have different ideas. It is your call. What is the risk for our team? All of your stories will be masked (i.e., “Team X”) unless you want to see your team’s name in lights. No team’s story will be shared without their consent with any external group (Eg MOHLTC) except in an anonymous way as part of the collected stories from the study. Why don’t we just go to the literature to find out what the enablers of Quality improvement are? We would love to. If you have suggestions of studies we should look at, please tell us! So far, most studies about “high performing teams” describe the way teams work but don’t compare that to a measure of performance. Teams are identified as high performers mostly by self-report or nomination by peers. Teams that self-report as high performers may or may not be the same as those with high performance on measures of quality such as those in D2D. Other studies identify high performers on the basis of administrative data (eg cancer screening rates, readmissions etc). These indicators do not reflect the overall quality of care provided nor the contribution of the team, which is problematic, given the interest in high performing teams. This study addresses those gaps by comparing team characteristics (such as those examined in other studies) with demonstrated ability to improve over several iterations of D2D (which we define as “high performance”). What is a “high performing” team? This study focuses on enablers for improvement. That means high performance is defined as “demonstrated improvement in D2D indicators over time”. D2D indicators reflect the patient perspective (patient experience survey indicators), the provider perspective (eg cancer screening etc) and the system perspective (e.g., readmissions). This is not a perfect definition of performance. It is, however, the most broad, current and ongoing source of primary care performance data available to describe the performance of primary care teams.
Standardized HbA1C targets do not take into account the complexity and diversity of our patient populations. Even targets that vary by age may not be sufficiently flexible; for example, a frail elderly person should have a higher target than a relatively robust person, even if their age is the same. Developing individualized targets that treat patients as individuals with unique circumstances and needs allows us to ensure that we are delivering the right care to each patient.
Better measurement of diabetes care
Simply put, using individualized targets allows us to count how many patients are getting the right care for diabetes, not just how many are meeting an arbitrary standard. One doctor noticed that in her own practice, only 65% of her patients met the standardized target of 0.07% HbA1C. However, when the metric was applied to individualized targets, 71% of her patients were at target. Indicators based on standardized targets fail to reflect the patients who are receiving the right care, when the right care means meeting an HbA1C level that is higher than the standardized target.
How?
Several teams have been working on tools to enable the recording and tracking of individualized HbA1C in their EMRs. Some of these are available for use now, and others are still in testing.
Denis Tsang, RD at CareFirst FHT, has developed an Encounter Assistant with two checkboxes for HbA1C targets: A1C <0.07 or A1C 0.071-0.085. Clinicians can check off either box after discussion with the physician responsible for determining the patient’s target. The individualized target is then appended to the patient’s cumulative patient profile and visible to all care providers. It is available for download from the Telus Community Portal.
Kevin Samson, Physician IT Lead, and Hope Latam, former QIDS Specialist, East Wellington FHT, developed a diabetes-management dashboard which works directly within Telus PS EMR. It provides a summary of each patient’s diabetes management and functions as a “report card” that the doctor can share with the patient. It provides at-a-glance data for the patient’s most recent HbA1C and other diabetes care indicators (creatinine, cholesterol). When an indicator is not within the target range, it shows up in red. By default, the dashboard uses standard targets (e.g., 07% for HbA1C), but a clinician can easily override this with an individualized value that reflects the right care for that patient. Once this is done, the form will compare the most recent HbA1C value against the individualized target to determine whether the patient is in or out of target. It is currently in testing at two FHTs and will be shared with other users of Telus Practice Solutions once complete.
Consider raising this as an issue at your EMR Community of Practice, and pressure your vendor to develop a solution. Meanwhile, clinicians can use the “notes” field to start recording individualized HbA1C targets in each patient’s chart. See if your team can agree on a consistent format for this, so any team member can recognize it easily.
Primary care teams are doing better than most in diabetes management. And what’s more, we’re getting better faster than most. This might not be that surprising to AFHTO members, almost all of whom have well-developed diabetes programs. What might be a bit of a shock is how far we have yet to go. While about 60% of patients with diabetes might meet at least one aspect of the guidelines for care, only about 10% meet the targets for a more comprehensive group of the key metrics: appropriate frequency of testing and levels of blood sugar and blood pressure, and appropriate prescription of statin for cardiovascular protection (pers. comm., K. Tu, 2015). It seems improbable that AFHTO members can’t do better than 10%, especially since some teams already are. AFHTO has already had success in working together to MEASURE primary care. We can take this one step further and work together IMPROVE care. To that end, the QIDS Steering Committee, in conversation with the board of AFHTO, have identified diabetes care as a priority to advance IMPROVEMENT of primary care across AFHTO. You can be part of this in the following ways:
Get up close with your peers.
Get up close with your data.
Get close to help.
Get up close with your peers:
Take a second look at presentations by your peers at the AFHTO conference and/or share your team’s approach to diabetes management.
Connect with peers about diabetes program planning, setting objectives and measuring progress, including selection of consistent indicators as outlined in the Schedule A indicator catalogue (available at the same link as the program planning information, above).
Consider using the data-capture tools for Diabetes outcomes being developed by the Diabetes Community of Practice. Contact your QIDS Specialist or AFHTO QIDS Program Staff for more information.
Sign up for CPCSSN or EMRALD to get ongoing, patient-specific reports to help you help your patients manage their diabetes.
Start using the D2D Diabetes Care queries – they reflect the performance of your patient population across a number of care processes (testing frequency and results of HbA1c and Blood pressure, statin medication for cardiovascular protection):
Increasing robustness of D2D diabetes indicator in D2D 4.0
Prior to D2D 4.0, the composite indicator used three measures for diabetes – this is inadequate. Additional indicators were added to integrate process and outcome measures and thus increase the robustness of the composite indicator. The intended result is an increasingly more meaningful tool to assess, measure, and compare quality of diabetes care. AFHTO members considered a number of indicators, based on their importance in clinical management of diabetes, scientific soundness, and feasibility. The following indicators were shortlisted. They are based on the latest guidelines from the Canadian Diabetes Association, Health Quality Ontario’s (HQO) Primary Care Performance Measurement Framework (PCPMF) and consultations with QIDS Specialists, clinicians and members of the AFHTO diabetes community of practice.
Percent of people with diabetes and LDL-C ≥ 2.0 mmol/L who are on statins.
Percent of people with diabetes who received a retinal eye exam in the past two years.
Percent of people with diabetes who received at least one peripheral neuropathy screening in the past year.
Percent of people <80 years old with diabetes whose HbA1C ≤7.0% in the past year.
Percent of people with diabetes with HbA1C levels at their individualized target (i.e.,≤7.0% or 7.1-8.5%).
Percent of people with diabetes who are confident in their ability to manage their condition.
The one indicator chosen to be added to the composite diabetes care indicator was percentage of patients with diabetes aged 40 years and older who have been prescribed a statin therapy. It is derived from the first indicators short-listed but modified for alignment with the most recent Canadian Diabetes Association guidelines.
Get close to help:
Bump up your QI skills with instructional videos from the University of Toronto Family Medicine department.
Tap into external resources to support clinical process changes such as those from HQO or others (check with your QIDS Specialist).
This list of resources is a start. We will be adding to it – keep checking back and adding your stories. Together, AFHTO members are changing the game of measurement in primary care. The time is right to build on this collective momentum to move beyond MEASURING to actually IMPROVING care.
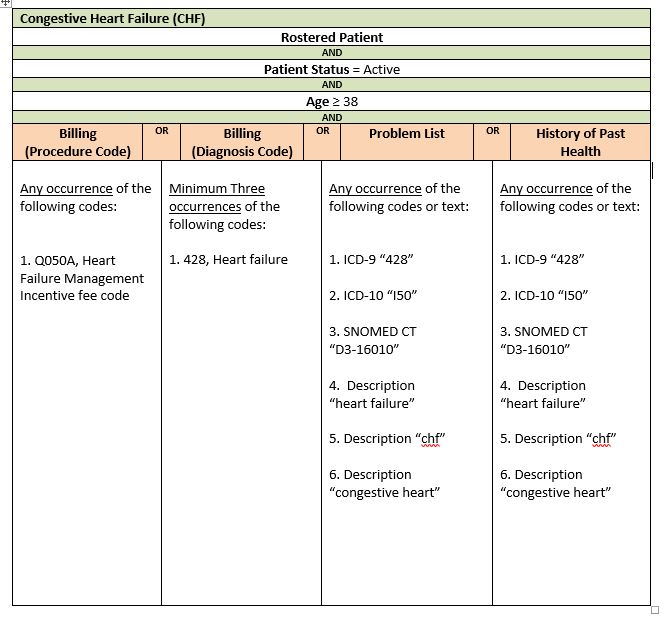
AFHTO has developed a standardized query to help you build a chronic disease registry for patients with Congestive Heart Failure (CHF) in your EMR. A chronic disease registry is an important step towards identifying – and ultimately correcting – gaps in care. The instructions below will help you get started.
Why CHF?
Congestive heart failure is the leading cause of hospitalization among older Canadians. It also is the most common cause of re-admissions to hospital. Being able to identify CHF patients can help you help them stay healthier and out of hospital as much as possible. This is good for patients and for the healthcare system, which spends nearly half a billion dollars on CHF care every year. The CHF query is intended for teams that do not yet have a reliable list of CHF patients. It will help you identify these patients if you don’t have the time or resources to start from scratch in reviewing all your patients Right now, the query is only available for teams with PSS or Accuro. (Work is continuing to expand the standardized query to OSCAR and Nightingale). Our CHF search tool has been built from the ICES EMRALD case definition, and then tested, revised, and validated using the eHealth Centre of Excellence EMR environment. This search does not require any data cleaning prior to use. The search process is reasonably accurate in that if it identifies 100 patients, 74 of those patients will actually have CHF. In a typical primary care practice of about 2000 patients, the search will likely identify 60. You will still have to review these 60 patient charts to be 100% sure (vs. 74% sure) which ones actually have CHF. However, this is much less work than reviewing all 2000 patients!
Query Criteria
Steps to complete your query
The following steps will help your team use the query to generate a list of CHF patients, starting from your EMR.
Step 1. Estimate how many patients you think this will affect. Multiply the number of patients your team serves by 0.03 (the estimated rate of CHF prevalence in Ontario) to get a rough idea of how many of your patients likely have CHF. If the resulting estimate is a manageable and meaningful number of patients for your team to build a registry of, carry on to step 2.
Step 2. Import the query into your EMR. Right now, you can only do this if have either Telus PSS, QHR Technologies Accuro or OSCAR EMRs. You will likely need the help of your QIDSS, IT staff or other person who usually works with your EMR to do this.
For PSS, click here to import the PSS SRX file into your EMR
Step 3. Run the query in your EMR. Again, you might need the help of your QIDSS, IT staff or other person who usually runs queries in your EMR. Running the query will produce a list of patients with CHF. The list will not be perfect – probably 25% of the patients identified by the query will NOT have CHF. The query gets you STARTED in building the CHF registry but doesn’t do the whole job for you.
Step 4.Find the patients who might not have CHF. Review the list of patients generated by the query to separate out those patients that are clearly already coded as having CHF. What’s left will the list of patients who MIGHT have CHF based on other data in the EMR besides formal coding.
Step 5. Prepare your physicians to review the list. Subdivide the list of possible CHF patients into separate, shorter lists for each physician. Work with your physicians to find out if they would prefer a list on paper or electronically and how they might like it sorted (i.e., by name, most recent visit, some other parameter).
Step 6. Invite each physician to review their list of patients. They know their patients best and can likely quickly confirm which ones do or do not have CHF, even though that information might not be easy for others to find in the EMR.
Step 7. Clean up your EMR data. Add CHF codes to the EMR for each patient that the physician confirms as having CHF. This so-called “data cleaning” work is a great job for a student. AFHTO has created a toolkit to assist members in recruiting and using students for data clean-up. Click here for the toolkit.
Step 8. Re-run the query. After you have corrected the EMR, re-run the query to generate a list of patients with CHF. This is your new CHF patient registry. Going forward, you can run the query anytime you need to generate a list of CHF patients. You can use the list to invite patients to a lung health program, track progress with outcomes on these patients once you have started such a program or any other purpose. Once you have identified them, recruit patients to your CHF program to improve patient prognosis, management, and overall care. Here are some example outcome measures to apply for these identified patients:
% of patients with CHF identified have action plans completed
% of patients with CHF identified are seen once a year to complete flowsheet
% of patients with CHF identified who’ve been hospitalized
% of patients with CHF identified who’ve been readmitted to hospital
For assistance and resources in setting up a care program for patients with CHF contact Karen Harkness at the Cardiac Care Network. This query was developed by QIDSS with assistance from eHealth Centre of Excellence, in support of all AFHTO members.
Information on this indicator related to D2D 3.0 can be found here. For technical notes, please see page 45 of the Data Dictionary.
Interpretive Notes
Tips to help you understand the data and put it in context.
Data Quality Actions
Tips to help you understand the quality of your data and, if necessary, take steps to improve it.
Potential Actions Related to Processes of Care
Concrete steps you can take to improve care, based on your data.Assuming you have established that the data are good enough to direct action AND that improving performance in this area is a priority for your team, you may wish to discuss the following options with your clinical leaders, Quality Improvement committees, team staff and/or patients:
In January and February of 2016, we conducted a series of focus groups with AFHTO-member Interprofessional Health Care Providers (IHPs) about what you need in order to get better at what you do – and about how we can get better at helping you with that. We heard a lot of great information from these focus groups! Now its our turn to teach back in order to be sure we heard right from all those who were able to be a part of the focus group discussions, as well as to get input from the wider group of volunteers to help us set priorities for action. To do this, we have created an anonymous, online survey. This brief questionnaire is your opportunity to tell us what Quality Improvement (QI) means to you, whether that’s even an accurate term to describe the process of getting better at what we do, and how we can support you in doing this. The questions for this survey come out of our discussions at the focus groups. Please confirm/correct our impressions and tell us which aspects of the enablers and barriers are the highest priority for you so they can also be the highest priority for our work together. Data from the focus groups and this survey will be used internally to set priorities in supporting teams to move beyond measurement to improvement. We can’t promise we will do everything that you identify as important – but at the very least, we can commit to focusing whatever resources we have in that direction. Data from the survey will also be used externally via direct communication and broader publication to advocate for resources/tools/other supports for AFHTO members. The results will also constitute part of the data being considered in my (i.e., Carol Mulder) doctoral thesis. Rest assured that your survey data will be completely anonymous, even to us – we won’t know who has completed it The survey has been sent to everyone who signed up for the focus groups. We look forward to learning from your responses and using them to help us in improving our efforts to help you. Thanks again for taking the time to share.
March 3, 2016
Thanks to the more than 100 IHPs who have signed up for focus groups!
What’s next?
Meeting invitations have now been sent for sessions in London (March 24), Toronto (March 29) and Kitchener (March 30). Planning for sessions in other locations is still underway. Not all IHPs will have received a meeting invitation; they were sent to those who indicated availability for the chosen date/time. Where there were more IHPs available than space in the focus group (maximum size of 8), a random sample of available IHPs was invited to the session. Closer to the dates of the sessions, we will send the high-level questions that will be addressed during the focus groups. There is no presentation planned as the goal of the sessions is to hear from IHPs about quality improvement, what it looks like in their teams and what it would take to better support it. All IHPs (not only those who take part in the focus groups) will be invited to comment on the guidance emerging from the focus groups and implications for AFHTO. To do that, we are hoping all IHPs who have signed up will agree to be added to the email distribution list for updates – watch your email for more information. AFHTO will work with all members to develop activities, resources and/or tools to support quality improvement within teams. These interventions will be informed by the focus group discussions and reflection on them by IHPs as well as other staff of AFHTO member organizations.
All IHPs are invited to participate in a series of regional focus groups. AFHTO has been making progress with measurement of comprehensive, team-based primary care. There is still more work to do with that. In the meantime, it is time to look beyond measurement to improvement in interprofessional care. IHPs are invited to complete the online survey about potential dates, times and locations as soon as possible so we can set up the sessions. We are looking for up to 6 people for each session on a first come, first served basis. The sessions will be facilitated by Lori Chambers, a qualitative researcher and doctoral candidate from McMaster and Carol Mulder, Provincial Lead for AFHTO’s Quality Improvement and Decision Support program. There is no charge for the sessions, which are expected to be about 1.5 hours long. Date and location of groups will be decided based on response to Doodle polls. The first sessions (which we anticipate to be in late March) will be held in the locations which fill up first. Additional options will be offered after the first sessions are set. Contact Carol Mulder for more information
Get even better at tracking how well your patients with depression are doing.
You can use the EMR tools shown below to get even better at tracking how well your patients with depression are doing.
Why do we need to do better?
Depression affects about 5% of adults in Canada each year and double that (i.e., 12%) at some point in their lives[i]. ALL Canadians are affected by depression, even they don’t have the disease themselves. This is because depression costs the Canadian economy at least $32.3 billion each year[ii]. In spite of this, people still have real fears of what people around them (families, friends, people at work, etc.) would think of them if they asked for help with depression. This keeps many people from asking for this help. This is where primary care teams come in. They have long term relationships with patients and can work with them to find the best ways to help them with their health.
What can we do to get better?
We can start by making sure we know which patients have depression. If you have a list of all patients that have depression, it will be easier to make sure all the right people are invited to the programs, with less risk of people falling through the cracks. The search tools below can help you find which patients in your EMR are likely to have depression.
What if I already know which patients have depression?
You might not need to use this tool if you already have a good list of patients who have depression in your EMR. The search is meant for teams that do not yet have a list of patients with depression and do not have a way to check the records of all their patients to come up with such a list.
How good is this search tool?
The search tool was based on the case definition from CPCSSN and the input from experts in depression at Hamilton FHT and St Michaels’ Hospital. The tool has been tested with the help of the eHealth Centre of Excellence EMR environment. The search gives few false negatives but does give some false positives. For every 100 patients that the search finds in your EMR, 62 patients will actually have depression but 38 might not. That means you will have to check the list of patients found in your EMR to be sure that they really do have depression. For a team with 10000 patients, you would likely have 500 patients to review. This is better than looking at all 10,000 patients – or not looking at any at all.
Which EMRs does the search work on?
Searches are available for TELUS PS, OSCAR, and Accuro EMRs.
How much data cleaning do I need to do first?
You do not need to clean your EMR data before you use the tool. The testing was done on EMR data as they are right now, for better or worse, so you can be sure there is a good chance it will help you too. You can just load it into your EMR and run it – ie it is plug-and-play. [i] 5% of Canadians 15 years or over affected by depression any given year. 12% of Canadians affected by depression over their lifetime. Statistics Canada’s 2012 CCHS. [ii] The Conference Board of Canada: Annual costs of depression due to lost productivity.
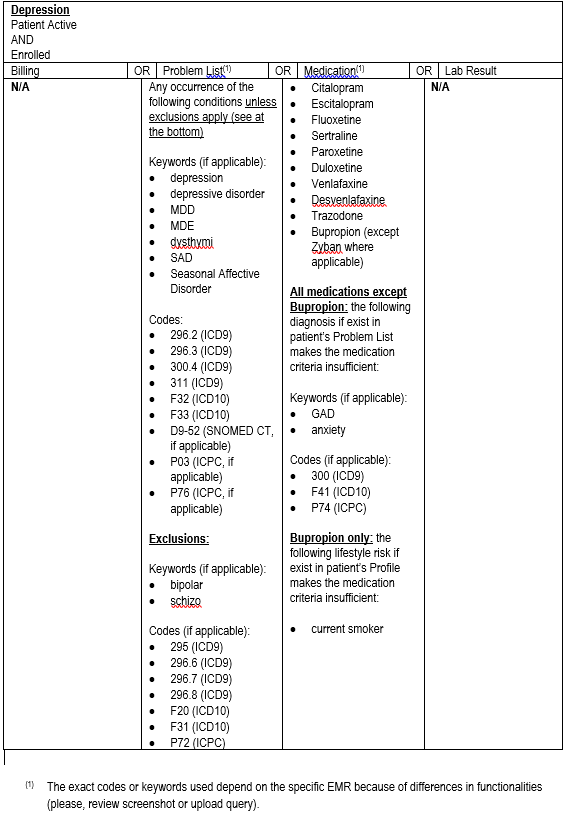
Technical details of the Query Criteria
(click image to see larger version) The Depression query is intended for teams that do not yet have a reliable list of patients with depression and don’t have the time or resources to start from scratch in reviewing all their patients to generate such a list. Right now, it is also only for teams with PSS or Accuro although work is continuing to expand the standardized query to OSCAR and Nightingale. The following steps will help your team use the query to generate a list of CHF patients, starting from your EMR.
Step 1. Estimate how many patients you think this will affect. Multiply the number of patients your team serves by 0.05 (the average rate of depression in Ontario) to get a rough idea of how many of your patients likely have depression. If you still think this is a big enough group of patients for you to generate a registry for, carry on to step 2.
Step 2. Import the query into your EMR. Right now, you can only do this if you have either Telus PSS or QHR Technologies Accuro EMRs. You will likely need the help of your QIDSS, IT staff or other person who usually works with your EMR to do this.
This document provides the query case definition information
Here you can find a guide on how to download the query
For OSCAR, please click here to download the numerator and denominator queries
Step 3. Run the query in your EMR. Again, you might need the help of your QIDSS, IT staff or other person who usually runs queries in your EMR. Running the query will produce a list of patients with depression. The list will not be perfect – probably 38% of the patients identified by the query will NOT have depression. The query gets you STARTED in building the depression registry but doesn’t do the whole job for you.
Step 4. Find the patients who might not have depression. Review the list of patients generated by the query to separate out those patients that are clearly already coded as having depression. What’s left will the list of patients who MIGHT have depression based on other data in the EMR besides formal coding.
Step 5. Prepare your physicians to review the list Subdivide the list of possible patients with depression into separate, shorter lists for each physician. Work with your physicians to find out if they would prefer a list on paper or electronically and how they might like it sorted (i.e. by name or most recent visit or some other parameter).
Step 6. Invite each physician to review their list of patients. They know their patients best and can likely quickly confirm which ones do or do not have depression, even though that information might not be easy for others to find in the EMR.
Step 7. Clean up your EMR data. Add depression codes to the EMR for each patient that the physician confirms as having depression. This so-called “data cleaning” work is a great job for a student. AFHTO has created a toolkit to assist members in recruiting and using students for data clean-up. Click here for the toolkit.
Step 8. Re-run the query. After you have corrected the EMR, re-run the query to generate a list of patients with depression. This is your new depression patient registry. Going forward, you can run the query anytime you need to generate a list of patients with depression. You can use the list to invite patients to a depression program, track progress with outcomes on these patients or any other purpose.
Step 9: Recruit patients to your depression programs. We will soon be posting resources in setting up a care program for patients with depression.
Step 10: Measure progress with patient prognosis, management, and overall care. Here are some example outcome measures:
% of patients who show an improvement in PHQ-9 score.
% of patients who show improvement on CES-D.
% of patients hospitalized.
% of patients with action plans.
% of patients self-identifying as satisfied after a group session.
This query was produced by and for QIDSS with assistance from eHealth Centre of Excellence in support of all AFHTO members. If you have any questions, please contact improve@afhto.ca.
The biggest news coming out of D2D 3.0 is the concrete data that higher quality comprehensive, patient-centered care is related to lower healthcare costs.
In addition to showing teams how they compare to their peers, D2D is making it easier for AFHTO to advocate for how team-based primary care could be measured across the province. With all the data submitted by members, we can show that measuring in a way that is meaningful and manageable for front-line providers makes a difference.
What difference does this make to your team?
Perhaps you and your team will be encouraged to hear the good news that high quality care is related to lower health system costs. The work you put into quality improvement does make a difference. You may also be encouraged by the early evidence from D2D (consistent with other published literature[1] ) that AFHTO members deliver better quality than the rest of the province on average. The comparison is not totally valid (because of differences in data sources and patient demographics) but it IS a comparison that many are interested in making. AFHTO is using D2D data to support arguments for a provincial solution for consistent capture of patient experience data as well as easier, more timely access to other important data sources. Finally, you and your team may also be encouraged that AFHTO now has an even more compelling argument for aligning performance in primary care with what really matters to patients and primary care teams. In the meantime, you may find the quality roll-up indicator useful at the local level (select the “Roll-up” tab at the top of the display). We have put together some tips for using your results to focus improvement efforts. And if you’d like to spread the good news around, consider sharing this handout with your colleagues. [1] Kiran, T., Victor, J., Kopp, A., Shah, B., & Glazier, R. 2014. The Relationship between Primary Care Models and Processes of Diabetes Care in Ontario. Canadian Journal Of Diabetes, 38(3), 172-178.