Get even better at tracking how well your patients with depression are doing.
You can use the EMR tools shown below to get even better at tracking how well your patients with depression are doing.
Why do we need to do better?
Depression affects about 5% of adults in Canada each year and double that (i.e., 12%) at some point in their lives[i]. ALL Canadians are affected by depression, even they don’t have the disease themselves. This is because depression costs the Canadian economy at least $32.3 billion each year[ii]. In spite of this, people still have real fears of what people around them (families, friends, people at work, etc.) would think of them if they asked for help with depression. This keeps many people from asking for this help. This is where primary care teams come in. They have long term relationships with patients and can work with them to find the best ways to help them with their health.
What can we do to get better?
We can start by making sure we know which patients have depression. If you have a list of all patients that have depression, it will be easier to make sure all the right people are invited to the programs, with less risk of people falling through the cracks. The search tools below can help you find which patients in your EMR are likely to have depression.
What if I already know which patients have depression?
You might not need to use this tool if you already have a good list of patients who have depression in your EMR. The search is meant for teams that do not yet have a list of patients with depression and do not have a way to check the records of all their patients to come up with such a list.
How good is this search tool?
The search tool was based on the case definition from CPCSSN and the input from experts in depression at Hamilton FHT and St Michaels’ Hospital. The tool has been tested with the help of the eHealth Centre of Excellence EMR environment. The search gives few false negatives but does give some false positives. For every 100 patients that the search finds in your EMR, 62 patients will actually have depression but 38 might not. That means you will have to check the list of patients found in your EMR to be sure that they really do have depression. For a team with 10000 patients, you would likely have 500 patients to review. This is better than looking at all 10,000 patients – or not looking at any at all.
Which EMRs does the search work on?
Searches are available for TELUS PS, OSCAR, and Accuro EMRs.
How much data cleaning do I need to do first?
You do not need to clean your EMR data before you use the tool. The testing was done on EMR data as they are right now, for better or worse, so you can be sure there is a good chance it will help you too. You can just load it into your EMR and run it – ie it is plug-and-play. [i] 5% of Canadians 15 years or over affected by depression any given year. 12% of Canadians affected by depression over their lifetime. Statistics Canada’s 2012 CCHS. [ii] The Conference Board of Canada: Annual costs of depression due to lost productivity.
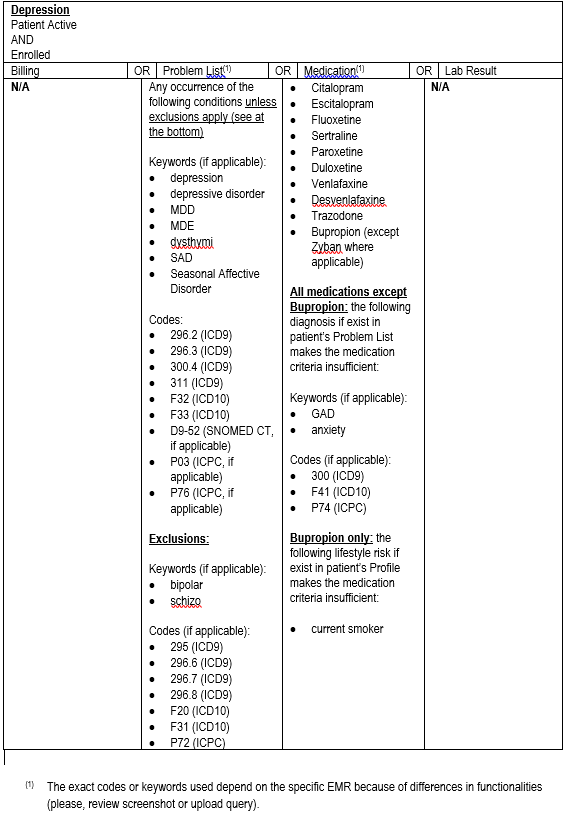
Technical details of the Query Criteria
(click image to see larger version)  The Depression query is intended for teams that do not yet have a reliable list of patients with depression and don’t have the time or resources to start from scratch in reviewing all their patients to generate such a list. Right now, it is also only for teams with PSS or Accuro although work is continuing to expand the standardized query to OSCAR and Nightingale. The following steps will help your team use the query to generate a list of CHF patients, starting from your EMR.
The Depression query is intended for teams that do not yet have a reliable list of patients with depression and don’t have the time or resources to start from scratch in reviewing all their patients to generate such a list. Right now, it is also only for teams with PSS or Accuro although work is continuing to expand the standardized query to OSCAR and Nightingale. The following steps will help your team use the query to generate a list of CHF patients, starting from your EMR.
Step 1. Estimate how many patients you think this will affect. Multiply the number of patients your team serves by 0.05 (the average rate of depression in Ontario) to get a rough idea of how many of your patients likely have depression. If you still think this is a big enough group of patients for you to generate a registry for, carry on to step 2.
Step 2. Import the query into your EMR. Right now, you can only do this if you have either Telus PSS or QHR Technologies Accuro EMRs. You will likely need the help of your QIDSS, IT staff or other person who usually works with your EMR to do this.
- For PSS, import the PSS SRX file into your EMR
- This guide provides instructions on how to import the searches into your EMR.
- Screenshots of the query can be found here.
- For Accuro, download the query “AFHTO Depression Frontend Search”from their publisher.
- This document provides the query case definition information
- Here you can find a guide on how to download the query
- For OSCAR, please click here to download the numerator and denominator queries
Step 3. Run the query in your EMR. Again, you might need the help of your QIDSS, IT staff or other person who usually runs queries in your EMR. Running the query will produce a list of patients with depression. The list will not be perfect – probably 38% of the patients identified by the query will NOT have depression. The query gets you STARTED in building the depression registry but doesn’t do the whole job for you.
Step 4. Find the patients who might not have depression. Review the list of patients generated by the query to separate out those patients that are clearly already coded as having depression. What’s left will the list of patients who MIGHT have depression based on other data in the EMR besides formal coding.
Step 5. Prepare your physicians to review the list Subdivide the list of possible patients with depression into separate, shorter lists for each physician. Work with your physicians to find out if they would prefer a list on paper or electronically and how they might like it sorted (i.e. by name or most recent visit or some other parameter).
Step 6. Invite each physician to review their list of patients. They know their patients best and can likely quickly confirm which ones do or do not have depression, even though that information might not be easy for others to find in the EMR.
Step 7. Clean up your EMR data. Add depression codes to the EMR for each patient that the physician confirms as having depression. This so-called “data cleaning” work is a great job for a student. AFHTO has created a toolkit to assist members in recruiting and using students for data clean-up. Click here for the toolkit.
Step 8. Re-run the query. After you have corrected the EMR, re-run the query to generate a list of patients with depression. This is your new depression patient registry. Going forward, you can run the query anytime you need to generate a list of patients with depression. You can use the list to invite patients to a depression program, track progress with outcomes on these patients or any other purpose.
Step 9: Recruit patients to your depression programs. We will soon be posting resources in setting up a care program for patients with depression.
Step 10: Measure progress with patient prognosis, management, and overall care. Here are some example outcome measures:
- % of patients who show an improvement in PHQ-9 score.
- % of patients who show improvement on CES-D.
- % of patients hospitalized.
- % of patients with action plans.
- % of patients self-identifying as satisfied after a group session.
This query was produced by and for QIDSS with assistance from eHealth Centre of Excellence in support of all AFHTO members. If you have any questions, please contact improve@afhto.ca.